This follows on from a prior question and discussion: Cable size between equipotential earth bonding bar and distribution board in a Group 1 medical location
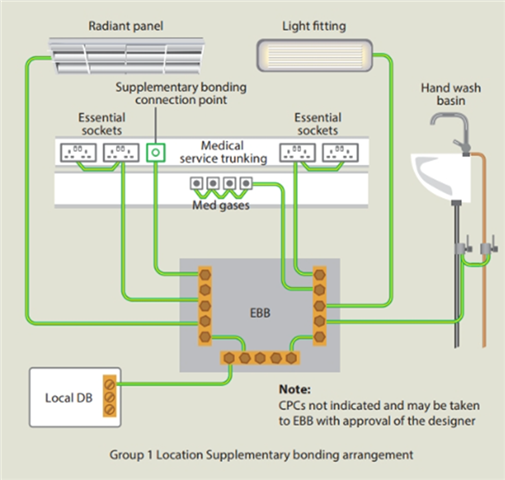
Regulation 710.415.2.3 states: The EBB shall be connected to the system earthing using a protective conductors having a cross-sectional area greater than or equal to the largest cross-sectional area of any conductor connected to the EBB.
Note HTM 06-01 provides no further definition of the point of connection of the EBB and the connection to the systems protective earth.
The clause is silent on the location; however, the consensus was: the local Distribution Board rather than the origin suffices.
Question 1 : The following statement has provided by a hospital engineer questioning this. Is this considered a user preference rather than regulatory compliance:
''Where practicable, medical equipotential bonding should be connected directly to the main earthing terminal to ensure integrity and clarity of the earthing system.
Risks of wiring EBB to a DB;
- Increased dependence on downstream connections
- Higher chance of unnoticed disconnection
- Harder inspection and fault tracing
- Greater lifecycle risk
- You are relying on the DB & MET connection
- Any future alteration, loose termination, or undocumented change can ;Increase impedance/break the bonding path
- The EBB is a safety reference, not just a CPC
- Increased impedance & higher touch voltages under fault conditions
- DBs are: Opened/modified/extended & re-terminated
- During future works: Earth Bars get disturbed/conductors get moved or resized/Temporary disconnections occur
- The medical equipotential system can be compromised without anyone realising
- Parallel earth paths and circulating currents cause issues with testing
Direct MET connection provides a solution that is as follows;
- Lowest risk
- Clearest compliance
- Preferred by healthcare AEs on a new project
Question 2 : From the statement above is this statement correct: The EBB is a safety reference and not just a CPC